The 3 Pillars of Wellness as a Service (WaaS): Human-Computer Integration, Redefinition of Health & Decentralization of Healthcare

For what’s already underway, there’s no existing community, event or even established industry category. Yet it represents a strikingly positive future and opportunity of health, computing and consumer technologies. I see it as on the same scale as the arrival of the personal computer.
We may be clouded in seeing it yet because of the tendency to see the new in terms of the old, in the same way that trains were initially seen as a way of pulling canal boats.
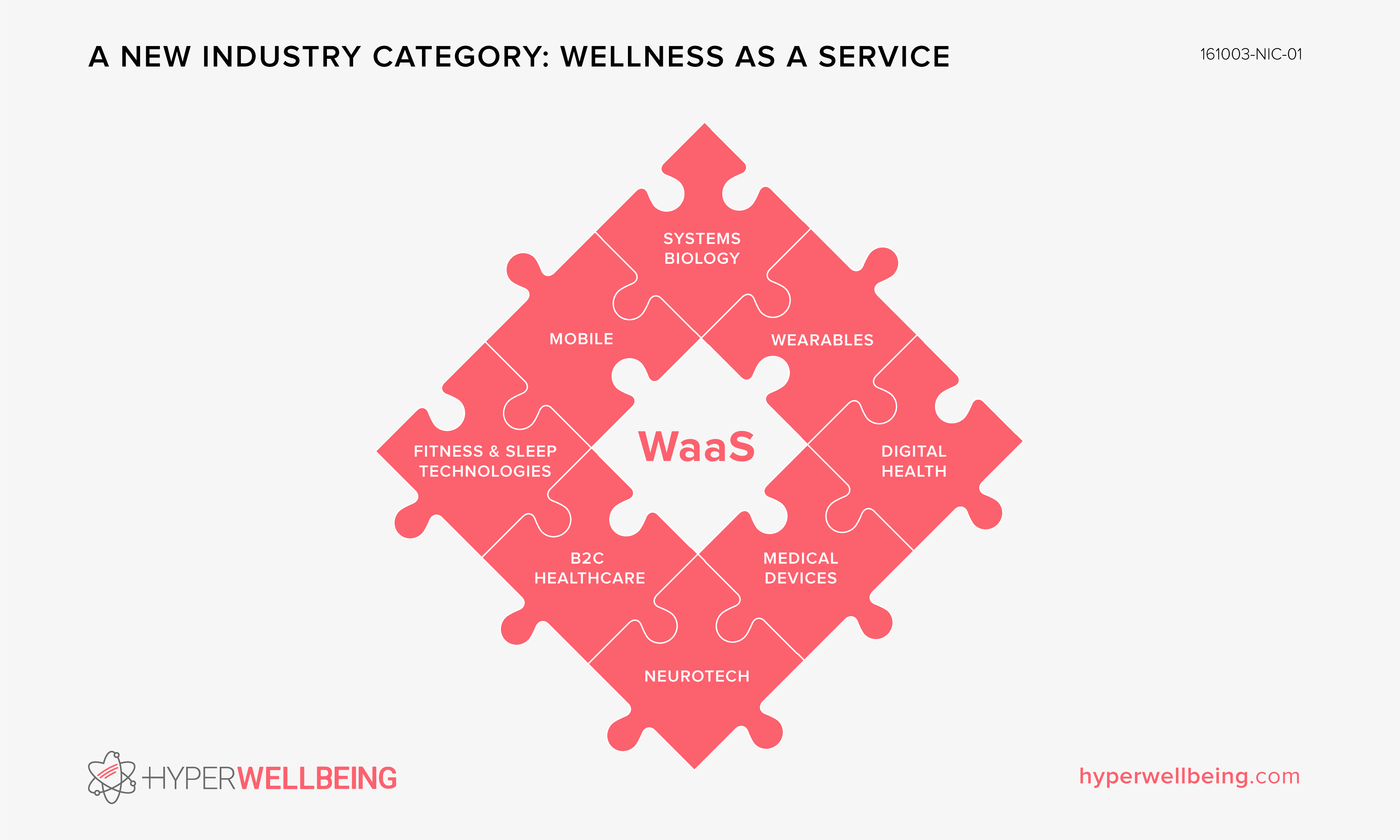
It’s not “digital health”, or “quantified self”, but is closely related, it is not “wearables” or “mobile”, although it’s the positive future of both. It’s not “connected health” or “health 2.0”, although it has relation. The best short-hand encapsulation is it’s a nascent industry, Wellness as a Service (WaaS). I think it will be one of the larger technological and cultural trends over the coming decade.
It rests upon three emergent pillars, each relatively equal. Before introducing these foundational pillars, it’s necessary to first state the current 100 word working definition of “hyper wellbeing”:
Hyper Wellbeing’ is focused on consumer technologies for data-driven health, wellness and life optimization, plus consumer data-driven disease risk reduction. The technologies are for ‘healthy’ individuals, who comprise the majority of the population. They are mostly smartphone and/or wearable based, or connected.It represents consumer empowerment, the future of computing and health. That future is an emerging Wellness as a Service (WaaS) industry. It will be financially driven not just by consumers but also health and life insurers, employers and corporate wellness programs. It dovetails the current consumerization of healthcare and its shift from a fee-for-service model to a fee-for-value model.
The three will interweave and multiply against each other to be greater than the sum of the parts as they enable WaaS, which as alluded to by name, is platform and consumer centric. I could label them as follows:
- Human-computer integration
- Redefinition of health
- Decentralization of healthcare
The first two pillars are quicker and easier to get an idea of, so I’ll cover them first.
Human-computer Integration
Human-computer integration is inevitable. If that’s not palatable we can simply switch the word “integration” for “convergence”. You can get more of an idea of it by reading “What is Hyper Wellbeing?” [1]. Approximately, computing has been moving from room size, to desktop, to pocket and now onto us. Within a decade the majority of us will be perpetually adorned and physically proximal to, “intimate” body/mind/lifestyle sensors, for example clinical grade biosensors and emotion detection circuitry.
It’s a pillar for three reasons. It’s responsible for producing the majority of a new class of data, “intimate data” (e.g. our vital signs, emotions, stress levels and so on). It’s the means of both conveying us insight about our bodies, minds and lives as well as co-opting lifestyle change etc. all via UX/UI. Finally although nascent, it will also be used to “write” back to the human being for example in the case of Thync, to lower stress and increase energy.
“Our most pressing health issues today are caused by the lifelong, daily dynamic interplay among our genetics, environment, and lifestyle choices. The solution does not lay in the form of a pill, syringe or medical procedure.” Lee S Dryburgh
Redefinition of health
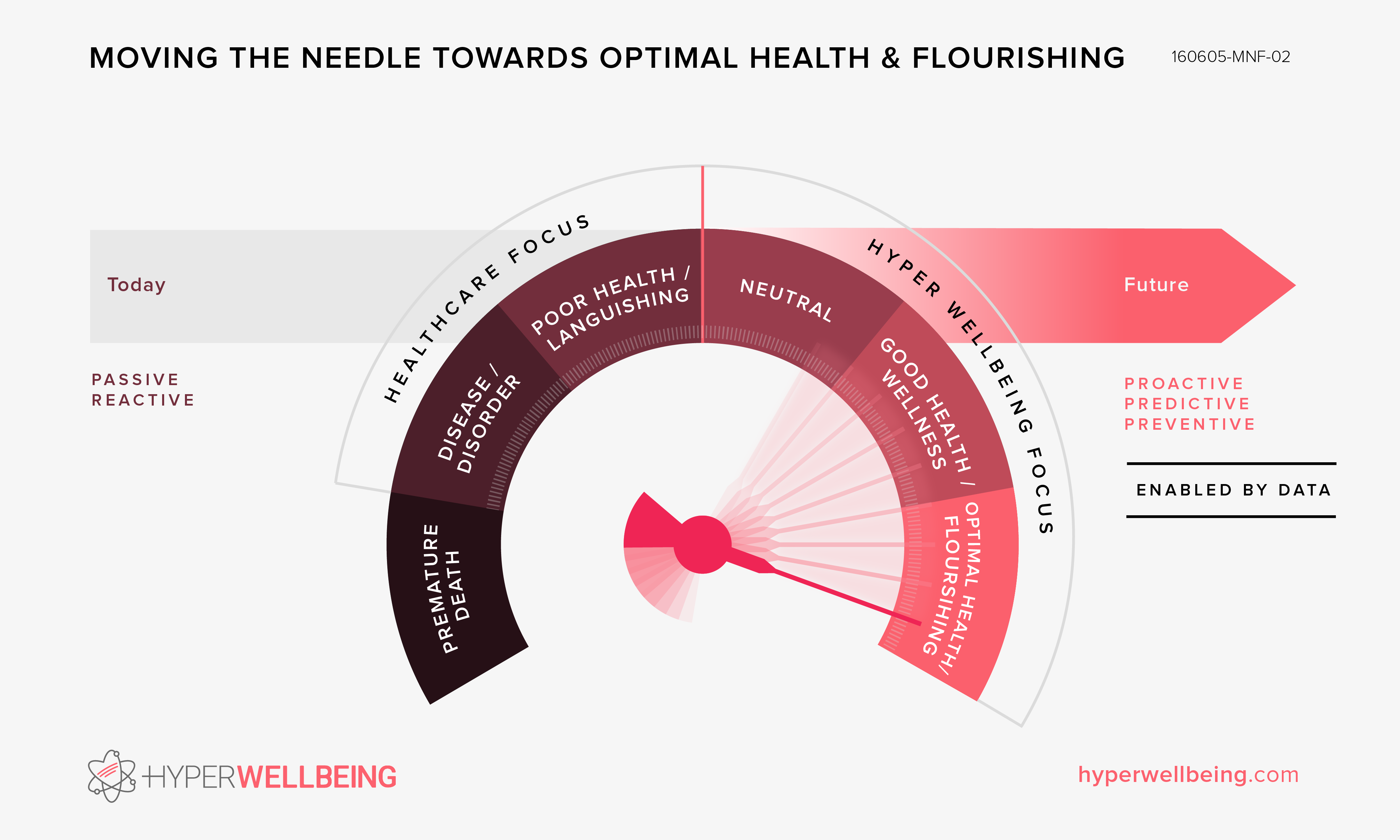
Today health is viewed as binary. We are simply classed as healthy or not healthy (“sick”). Our present day definition of health is “If you don’t have any apparent disease, and you look and feel OK, you’re healthy” [2]. It’s a definition which dates back to the 14th and 15th century. It’s predominantly only once one has already become sick that one enters the “healthcare” system where diagnostics are then performed, measurements are taken and a plan to manage or treat (if possible) the sickness is made.
This definition and paradigm is set to change over this coming decade. However the healthcare system will remain largely “sick care” focused although itself advancing (personalized medicine, A.I. driven diagnostics, “digital health” based remote patient monitoring etc.).
“In this society what we see is a society that literally makes people sick. Because 50 percent of north american adults have a chronic illness, either diabetes [3], or high blood pressure [4], or heart disease, or cancer, or any number of auto-immune illnesses. Now, according to the strict medical model, that is too bad, these people are just unfortunate, because what the medical model does, whether with mental illness or physical illness, it makes two separations, it separates the mind from the body, so that what happens emotionally is not seen to have an impact on our physical health. Number two it separates individuals from their environment. So that we try to understand individuals in separation from their actual lives.” Gabor Maté
The paradigm (and dollars) is likely to shift towards prediction, prevention and optimization. It will for the most part will be driven by consumer technologies and retail services, particularly working in hybrid (e.g. genetic and omics data derived from retail services combined with day to day physiological data and lifestyle guidance via mobile, wearables and other consumer electronics).
Craig Venter recently stated “It turns out that 40 percent to 50 percent of healthy people have serious and in some cases life-threatening disorders that they’re completely unaware of because they haven’t risen yet to the level of significance in their bodies where they’re causing symptoms.” [2]
““Performance-based allotment rate” shall be determined within the range of 0% to 100%.” NEC Corporation Meeting 2016
Leeroy Hood recently stated “the market cap of the scientific wellness industry will dwarf the current cap of the disease industry in as soon as a decade” [3] and “You may think that you’re well, but you can be a lot weller than you are right now” [4]. He said that in a pilot study of 108 outwardly healthy subjects, 91 percent of them had serious nutritional deficiencies, over 50% had health issues, such as chronic inflammation or pre-diabetes [4].
Decentralization of Healthcare
What is starting to take place in healthcare parallels what has already taken place a decade before in telecoms. In that case, telecom operators were the “institution”, the command-and-control hierarchy as opposed to something with more of a peer-to-peer networked topology and power structure. Innovation was stalled for decades because there was such an innovation gatekeeper. Operators decided what apps if any could be installed on “their” subscriber’s handsets or what “supplementary” services could be deployed. To attempt to get an app onto a mobile phone as a third-party (for the few operators open to the possibility) it would take many high-level executive meetings, much legal work and something of the order of a ~60K USD payment (around 2006).
“When you look at what’s happening with life science right now, it’s almost like watching the industrial revolution—but in fast-forward. Modern technologies for analyzing large-scale health care data offer unprecedented opportunity to provide a better quality of life, across the globe. How does health evolve not only year to year, but also day to day and even minute to minute? That’s what technology can help us understand. No matter how tech-savvy you are, we’ll make sure that setting up the devices feels like a breeze.”Google Ventures
As a result telecoms for decades witnessed little innovation except for the accidental creation of a popular service, short-messaging-service (SMS). Over these decades operators talked a lot about innovation (for example video calling each and every decade starting in the 1960s) and spent considerable money on a never-ending stream of relatively failed “innovation” initiatives. It’s questionable whether there had been real interest in service/application innovation because they had very strong cash cows of voice minutes and later messaging. Most innovation would have been seen as a threat to this lucrative business model plus there was inherent inertia owing to the asymmetrical power structure in their favor.
Operators had the imbued attitude until only less than a decade ago that they controlled the subscriber experience, that they owned the subscriber, that they were source of innovation. It’s not a surprise given they had a 100+ year static history of operating a capital intensive network and renting it out to subscribers with dumb terminals.
Following the turn of the 21st century operators increasingly spoke with grandiosity of branching out into becoming media companies, software companies, and of collectively building a “better internet” although as a walled-garden in competition with the public internet and with much engineering work spent on micro-billing abilities.
However communications innovation increasingly appeared from the edges of the public internet instead. People were using email, partaking in multiplayer massive online games, photo sharing, using wikis, blogging, instant messaging, using chat forums – all creating a general sense that innovation was occurring on the internet instead and along with it, was starting to absorb the future of communications user experience itself.
In 2004 Skype began to rise to prominence. It was particularly interesting as it improved upon the core product of operators (voice) by offering high-definition audio, it was free of charge regardless of distance or time and it did not rely upon expensive components in the core network, instead it ran as a peer-to-peer network among the network edges (user’s computers). In 2006 YouTube launched offering global video distribution capabilities to anybody free of charge.
In late 2007 a computer manufacturer (Apple) launched a phone that was a pocket computer, later offering an SDK to make it “open” (anybody could write an app for it and disseminate it via Apple without upfront fees). The following year a search engine company (Google) launched a phone operating system similar to Apple’s. “App stores” appeared and innovation has went into hyper speed since.
The same narrative is starting to unfold for healthcare. We’re at the 2006 stage by comparison. This is when people were just beginning to create DIY phones, creating mobile Linux platforms etc. There is no “iOS/Android” of healthcare yet but it’s similarly brewing so to speak.
Telecom operators missed what was coming as they ignored the rising power of the edges of the network (owing to increasing processing, memory and connectivity). The same appears to be gathering for healthcare. It assumes it’s at the center of “health” and speaks only from a doctor-patient power relationship and a sickness paradigm (one side knowledgeable and capable of easing suffering and the other side sick and in need). Consumer technologies are advancing towards enabling a similar power-shift towards the network edges.
Just as the smartphone has unleashed innovation way beyond what we could have imagined when it was restrained within the institution of “telecoms”, the same will be true of WaaS, particularly when the two other pillars are taken into consideration.
Attempting to Peak Past a Decade Ahead
It’s hard to chart beyond the three pillars presently, particularly how the three will interplay and even harder still to envisage beyond a decade from now. But we can make some educated guesses.
Humanity finds itself suddenly with poor decision making “hardware” (the brain) for the present environment e.g. with electrification enabling night to become “day”, with dense calories available on demand without a pre-requirement of energy expenditure, with chronic stress etc. It’s why for example we’re attracted to foods and food combinations which cause chronic inflammation (a core driver of chronic disease).
Personal choices are now the leading cause of death [5]. Non-communicable diseases (the four main NCD are cardiovascular diseases, cancers, diabetes and chronic lung diseases) are the leading cause of death globally and accounted for 38 million, or 68% of the global deaths in 2012 [6].
Our most pressing health issues today are caused by the lifelong, daily dynamic interplay among our genetics, environment, and lifestyle choices. The solution does not lay in the form of a pill, syringe or medical procedure. It lays in increasingly available data owing to the first pillar (genetic, environmental and lifestyle) and data processing (e.g. Big Data and machine intelligence), the result of which will come to understand causations.
The insights will be used for example to augment human decision making, e.g. within five years your smartphone will suggest what you eat [7], when you sleep and for how long etc. It’s rather clear the next ten years is likely to be focused on consumer data-driven prevention and wellness optimization.
Beyond the five year mark, consumer technologies are likely to show practical progress beyond the lower “physiological” rung on Maslow’s hierarchy of needs [8] to higher rungs for example “love/belonging”, augmenting and facilitating our marriage (itself a key contributor to our health) and other relationships [9]. They’re even likely to augment our decision making on whom to marry in the first place. It’s likely that ambient AI systems such as today’s Alexa will “observe” our relationships, prompting us when we are violating “relationship science” (e.g. employing a defensive communication style) [10]. Ditto when we break “the science of happiness”.
But as we move beyond a decade, things extend past a “holistic individual health/wellbeing” view (e.g. systems biology, biopsychosocial model of health) towards a view which includes other systems in which we live e.g. political, economic and the biosphere.
Currency will become decentralized [11] and may evolve to put wellbeing at the heart of the economy itself unlike today where the economy has become disassociated from actual human needs (to the point that it actively aggravates human suffering in order to “profit” from the sale of “solutions”). Governance may also move towards decentralization, e.g. a networked “liquid democracy” [12], improving population wellbeing in the process. Ultimately we’ll move past “simply” optimizing the lifetime of the individual, towards optimizing life on Earth. That means making real-time optimal choices based upon all of life on Earth, including making choices within sustainable ecological constraints.
Everybody wants health, wellness and optimal living. The future of wearables, mobile and other consumer technologies is aligning with those needs. In the distant future, our economy and systems of civic and planetary governance need to align.
Comments